



8,567
Choptank Patients Called
72%
Patients Engaged with Automated Calls
* Total Inpatient and ED Encounters Called
1 Hour
Median Follow-Up Time from Care Coordinators
38%
Engaged Patients Indicated an Issue Requiring Care Coordinator Follow Up
Choptank Community Health: Automated Outreach Reduces Readmissions for Underserved Patients
8,567
Choptank Patients Called
72%
Patients Engaged with Automated Calls
* Total Inpatient and ED Encounters Called
1 Hour
Median Follow-Up Time from Care Coordinators
38%
Engaged Patients Indicated an Issue Requiring Care Coordinator Follow Up
Choptank is a Federally Qualified Health Center (FQHC), on the eastern shore of Maryland, part of the Maryland Community Health System, servicing approximately 27,500 patients annually. Choptank continuously works towards their mission and vision of providing access to exceptional, affordable care that improves the health and well-being of their community.
PROGRAM BACKGROUND
As research demonstrates, post-discharge follow up plays a critical role in improving patient outcomes and experiences. For Choptank, they sought to find ways of providing effective follow-up to their patients after a hospital visit and needed a solution that could engage their patient population largely made up of Medicaid beneficiaries.
IMPROVEMENTS
Choptank implemented CipherOutreach to streamline patient engagement workflows. By directly integrating with Maryland’s State Health Information Exchange (HIE), CRISP, CipherHealth identifies patients needing follow up during their care transitions after a hospital visit anywhere within the state. Recently discharged Choptank patients receive automated calls asking about their care transition and status. Should a patient indicate an issue, Choptank care coordinators are notified and help to resolve the concern.
RESULTS
By proactively reaching out to patients with CipherOutreach, Choptank reduces the likelihood of adverse events and keeps patients from revisiting the hospital or emergency room. Within six months, Choptank made 8,567 calls and achieved an impressive 72% engagement rate. Patients who engaged with the follow-up calls were 37% less likely to experience a 30-day inpatient readmission and 38% less likely to experience a 7-day return after an emergency visit. Additionally, data collected through the program helps identify actionable improvements to bring patients back into care in the comunity, such as scheduling a PCP follow-up visit or connecting patients to other healthcare resources.
Comparing 30-Day Inpatient Readmission Rates and 7-Day Emergency Patient Readmission Rates for Engaged and Not Engaged Patients
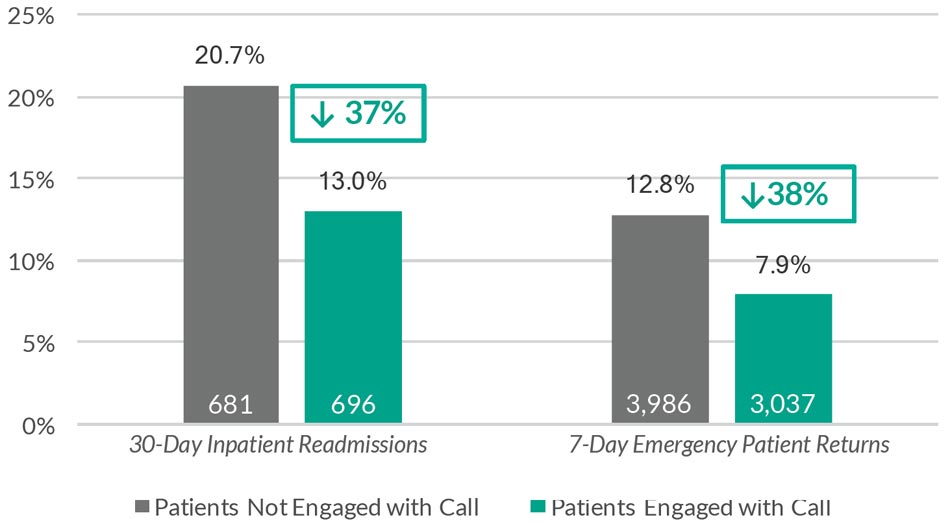
Some “Reason for Visit” encounters such as pregnancy/labor are excluded from the analysis
CLIENT: Choptank Community Health, PROFILE: Maryland-Based Federally Qualified Health Center (FQHC), PRODUCT: Post-Discharge Follow Up, PROGRAM: Care Transitions Outreach DATA PERIOD July 2017 – Jan 2018