




Contributors: Lyndsey Lord, M.B.A., R.N., Sheela Doraiswamy, M.P.H., Alyssa Kleinman
ABSTRACT
Patients receiving home health services may require assistance outside of their routine visits. Thoughtful engagement throughout the home health episode improves patient satisfaction and ensures patients remain on the path to recovery. This data analysis measured the impact of consistent patient engagement throughout a patient’s home health episode on patient satisfaction scores and re-hospitalization rates. The results demonstrated that increased engagement throughout the episode of care led to better outcomes and improved patient-reported experience. Further research is required to understand how the cadence of engagement opportunities impacts re-hospitalization rates and HHCAHPS scores.
INTRODUCTION
Home health services make up a significant portion of postacute care in the United States.1 As patients transition home following an acute or skilled nursing facility stay, the additional support provided by home health agencies is imperative to keep patients on their path to recovery. Even with the use of home health services, patients may require additional support in between visits to ensure they understand and are taking the proper actions to prevent adverse events such as a return to the hospital (re hospitalization).
Care in the home is rising, and the intensity of service and level of skills provided has expanded greatly. This expansion is driven both by consumerism and payment reform. Patients convalesce optimally in a familiar and comfortable environment, such as their home; this preference has prompted physicians and healthcare providers to collaborate with home health agencies to create structures and programs to manage sicker and more complex patients. Although patients receiving home health services will have the support of a visiting nurse, there are often issues such as medication adherence that arise outside of the scheduled home visits. Industry research has identified that concern or confusion on these items will often lead to adverse events or re-hospitalization; prompt resolution of these issues will ensure a patient is supported on their path to recovery.
As such, consistent engagement to reinforce plan of care, provide additional clinical education, and ensure necessary follow-up is an increasingly important strategy following a patient’s hospital discharge or following an emergency room visit.2 To ensure patients receive the support and care they need, communication between home health visits can be equally effective in keeping patients safe and satisfied.
CHALLENGES DURING AND BEYOND THE HOME HEALTH EPISODE
There are various patient concerns or issues that may arise throughout or following a home health episode of care. These challenges can impact the degree to which patients receiving home health services have adequate support to adhere to their care plan and remain on the path to recovery. This may include important education about their disease process, care plan, or recovery that may be misunderstood by patients and/or their caregivers. These issues, in addition to social determinants of health, such as patients’ socioeconomic status and physical living environment, can affect recovery throughout and following the home health episode.
In light of these industry challenges, this study was designed to better understand the impact that automated calls across a home health episode have on re-hospitalization rates and HHCAHPS scores.
THE STUDY
CipherHealth conducted a retrospective analysis to measure the effectiveness of consistent automated outreach on patient outcomes and experiences, as measured by re-hospitalization rates and HHCAHPS scores. The analysis was completed with one of CipherHealth’s client organizations, a home health and hospice agency with an average daily census of more than 5,000. Approximately 75% of the patients are Medicare beneficiaries.
The agency uses CipherHealth’s automated outreach technology to call patients throughout their episode of care and beyond. Patients will receive automated calls on behalf of the home health team five times throughout the home health episode of care and one time following the end of the episode. During these calls, patients are asked about symptom management, medication understanding, and follow up needs. In response to the questions, patients are able to indicate when they have a question, triggering a call back from a team member from the home health agency to address the concerns and resolve any issues.
STUDY APPROACH
This study required a re-hospitalization analysis in addition to an analysis of HHCAHPS respondents. The re-hospitalization analysis included 5,985 patients over a 9-month period. The patients were divided into two groups based on whether or not they had engaged with the automated outreach call. “Engagement with the call” is defined as “answering the phone and responding to at least one clinical question on one or more calls.” A total of 4,966 patients engaged with their call (83%), while 1,019 patients had not. Using data provided by SHP, a vendor that aggregates home health outcomes and quality metrics, this analysis investigated the level of engagement for re-hospitalized patients and compared with those who completed their home health episode without an unplanned admission.
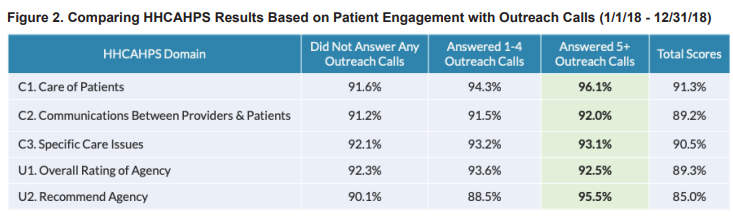
The HHCAHPS analysis included 1,026 survey respondents over a 12-month period, more than half of whom were also included in the automated outreach program. The patients who were part of the program were then split up into two groups based on call engagement, and the average Top Box score for the five different HHCAHPs domains were compared.
RESULTS
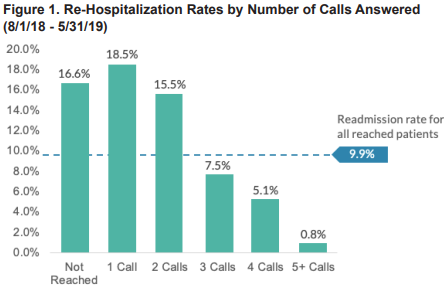
CipherHealth’s retrospective data analysis identified that patients who engaged consistently with the calls had a lower likelihood of re-hospitalization. Additionally, patients who engaged with five or more outreach calls recorded higher top box HHCAHPS scores in 3 out of 5 domains than patients that did not engage in the calls, including the domain “willingness to recommend the agency” (Figure 1).
This study suggests that it is beneficial to consistently engage patients throughout a home health episode to improve outcomes and experience. The automated calls allow patients multiple opportunities to communicate needs while providing the home health agency with the information and workflows necessary to help address patient concerns quickly. The home health agency team followed up on patient issues and concerns within three hours. This timely follow up contributed to the agency’s success, and is imperative within outreach programs to ensure that patients remain on the path to recovery.
REFERENCES
1. Institute of Medicine. The Future of Home Health Care: Workshop Summary.
Washington, DC: National Academies Press; 2015. http://www.nap.edu/catalog/21662
2. Rennke S, Nguyen OK, Shoeb MH, et al. Hospital-Initiated Transitional Care
Interventions as a Patient Safety Strategy: A Systematic Review. Ann Intern Med.
2013;158:433–440. doi: 10.7326/0003-4819-158-5-201303051-00011


